
In today’s world of genetic variations, dentists frequently come across kids who have congenitally missing lateral incisors, or incisors that are abnormally small (“peg” laterals).



The choices would be:
- Preserve or enlarge that space with braces.
- Do nothing and let nature take its course.
- Close the space up with braces.
This article is intended for the parent. What would YOU instinctively decide to do, if your child had missing teeth and there were spaces where there should be teeth? How about if there are NO spaces left, the teeth have just move in and closed them up?
Lara had one missing lateral on her right, and in her case the space was closed. There was one peg lateral on her left.



Dr. Sarkissians viewpoint, which is the most biologically sound one, takes into consideration ESTHETICS, JAW-JOINT HEALTH, AIRWAY INTEGRITY, AND AGAIN, FACIAL ESTHETICS.
Since Dr. Sarkissian strongly believes in maximum jaw size,
he has always chosen OPTION 1.
This option will be somewhat costlier, but in the long run it is so much more beneficial if you consider the disastrous consequences of NOT doing it. The time to act is WHILE the child is in the growth phase, between the ages of 7 and 15. This is the time when the bone is growing and can be influenced to develop faster with JAW ORTHOPEDICS.
The consequences of option 2 (doing nothing): Missing teeth cause a retardation of growth of the jawbone in that area and the front part of the jaw collapses. The arches holding the teeth will shrink, and the child will grow into an adult with a face that looks flat in the middle, will have flat lips with no support, will appear to have a LARGER NOSE, will suffer from TMJ problems (due to the lower jaw being trapped under the smaller upper jaw) and may even suffer from sleep apnea.
The consequences of option 3 (braces to close the spaces): This is like a death sentence for the healthy development of the child. Absolute negation of biological growth tendencies. Taking a small jaw size and making it even smaller by pulling teeth together goes against all developmental principles. Take all the damaging consequences Dr. Sarkissian has outlined above in option 2, and increase them ten-fold. When this child grows into adulthood, he/she will have the arch size of a 6-year old and a mid-face which is CAVED IN. At least in option 2 the arch size will achieve an equilibrium determined by tongue function on one side and pressure from the lips and cheeks on the other.
Dr. Sarkissian’s philosophy in treating Lara was, very briefly stated, as follows:
- Develop the jaw sizes, vertically (she had a deep overbite), and sideways, with arch development (her jaws were smaller than normal). (see Orthodontics)
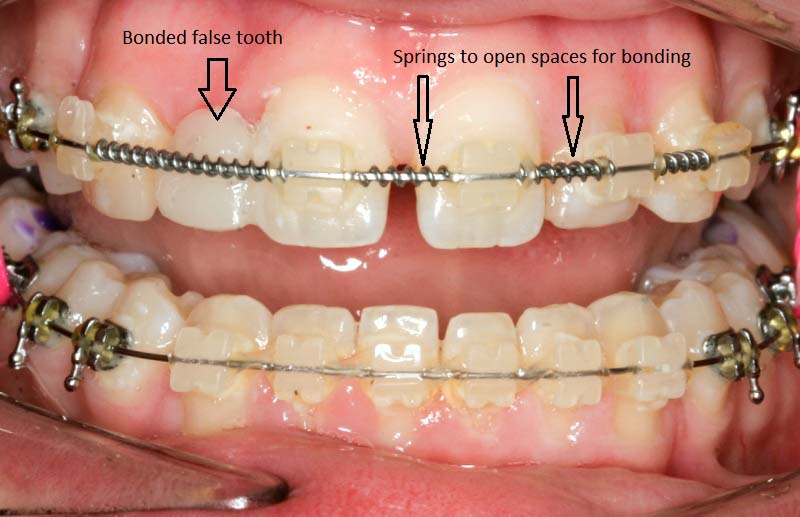
- Braces to align the teeth, to flare the upper incisors towards the lips, and to open the space where the lateral would have been, by pushing the canine backwards (This in itself allows us to gain arch length and size)

- Open the space around the peg lateral.
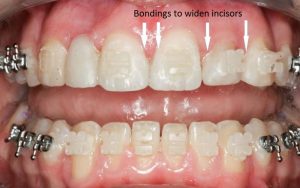
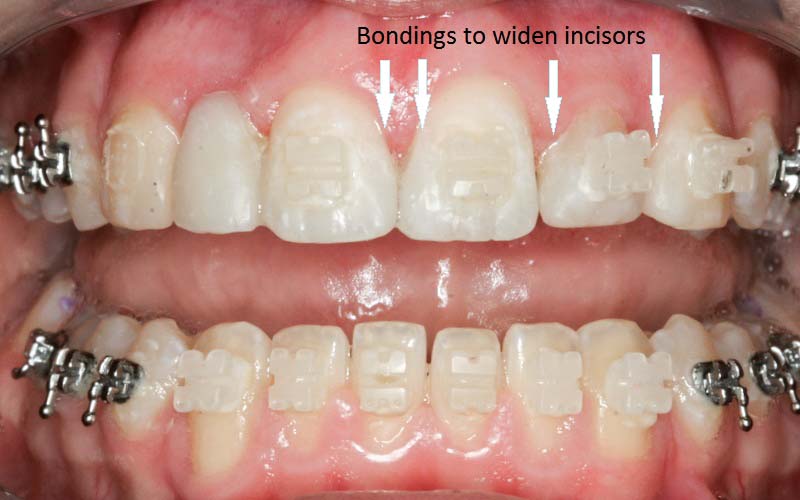
- Bonding of the peg lateral with composite to give it a wider look, in proportion to the central incisor, and to sustain the arch development. Dr. Sarkissian even bonded the central and canine teeth to make all of them wider, in proportion of course, for a maximum esthetic effect and to keep the teeth in a wider arch.
- On her right side, after the space was even with the space of the now-widened peg lateral, Dr. Sarkissian bonded a composite false tooth, attached to only one side, free on the other, to allow the teeth to independently move and settle. After the braces are completely finished and taken off, and after the retainer phase, the false tooth will be bonded to both sides similar to a fiberglass-retained “Maryland bridge” (see video) Once the child reaches 18, or anytime later, a ceramic implant would be an option.
Lara’s final photographs show an appealing profile, a wide, pretty smile showing a full set of teeth, and proper lip support. She still has the bonded tooth, which can be repaired anytime something happens, until she is ready to receive an implant, if at all.


